We guide healthcare professionals in a solution-focused approach so clients can embrace possibilities, opportunities, and a fresh vision for the future.
Deb and Tami are all smiles after our presentation at #ADCES22
August 12-15 brought us a fresh point of view in Baltimore, MD at #ADCES22! What an incredible conference, and so good to be back with friends and colleagues we haven’t seen in- person in 3 years.
We were honored to present to a full room late on a Friday afternoon! Our presentation highlighted 7 tactics for your toolbox, so to speak, to transform primary care visits.Since the majority of type 2 diabetes is managed in primary care, it seems the best place to start to change the way we engage with clients/patients is in the primary care setting. In case you missed the 7 tactics, and are wondering, here you go…
As we mentioned during our presentation, these tactics can largely be applied in other practice settings as well.
Celebrating with friends after our presentation
Stop back by in 2 weeks when we’ll share perspectives on embracing a “growth mindset” – a particularly impactful concept we learned about at the conference and one where, we believe, the tenets of a solution focused practice align.
View of Baltimore’s Inner Harbor
We welcome anyone interested in our approach to Subscribe to our blog and we’ll email you when a new post is published!
If you are a health care professional and interested in learning more about our solution-focused practice and approach, when you subscribe to our blog, we’ll send you in return a FREE resource of 10 Solution-Focused Questions to start a solution-focused discussion with your clients.
Follow us on Twitter and Instagram @AFreshPOVforYou
Deb is employed by Dexcom, but her words and opinions in this blog are her own.
Tami is employed by the University of Kentucky HealthCare Bar
Problem talk can create problems. Solution talk creates solutions. – Steve de Shazer, pioneer of solution-focused brief therapy
Our last blog wrapped up a series of posts on transforming primary care encounters by taking a solution-focused approach when managing type 2 diabetes in the primary care setting. This series has received overwhelming positive feedback. We were excited when an abstract we submitted on the topic to ADCES22 conference was accepted for presentation! If you will be attending the conference in Baltimore, we’d love to have you join us on Friday August 12 at 4:45 pm where we will share 7 tactics for your diabetes education toolbox to transform primary care visits. In large part, the tactics can be applied to other practice settings as well.
Without a doubt, managing diabetes is complex. We know that constant focus on “problems” can erode confidence. So clients/patients may turn to us, their healthcare team, looking for guidance to do something different. Stepping alongside our clients/patients as a “think partner” allows working together to identify solutions to move the individual forward towards achieving their health goals.
Implementing solution-focused tactics leads to greater individualization of care through a brief intervention. We’ll give you a sneak peek of what we’ll share in our presentation…
We’ll be discussing each of these, providing a multitude of practical tips to implement them, and provide real-life examples.
Action Plan for Change
1.Identifies solutions (instead of problems) and how to make the exceptions happen more often.
2.Focuses on doing more of things that are going well (not on doing new things).
3.Identifies small steps to take toward what is desired (instead of what is NOT wanted).
4.Identify strengths one has/uses to help manage diabetes every day.
5.Considers how positive thinking and action affects life.
6.Recognizes what worked.
Stop back by in 2 weeks when we’ll share our favorite behavioral sessions we attended at the ADCES22 conference!
We welcome anyone interested in our approach to Subscribe to our blog and we’ll email you when a new post is published!
If you are a health care professional and interested in learning more about our solution-focused practice and approach, when you subscribe to our blog, we’ll send you in return a FREE resource of 10 Solution-Focused Questions to start a solution-focused discussion with your clients.
Follow us on Twitter @AFreshPOVforYou
Deb is employed by Dexcom, but her words and opinions in this blog are her own.
Tami is employed by the University of Kentucky HealthCare Barnstable Brown Diabetes Center, but her words and opinions in this blog are her own.
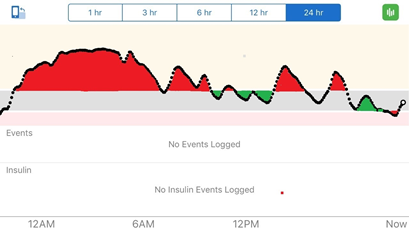
CGM tracing showing time in range (in green) and time out of range (in red)
The real voyage of discovery consists not in seeking new landscapes, but in having new eyes. – Marcel Proust
We kicked off 2022 with this series we’re wrapping up today: Transforming primary care encounters by taking a solution-focused approach when managing type 2 diabetes in the primary care setting. Along the way we’ve shared a multitude of tips and tactics to add to your toolbox so speak. Today’s blog wraps up the series as we focus on discovery learning from diabetes data in a solution-focused way.
While there is a multitude of diabetes data that we can learn from, today we’re focusing on structured blood glucose monitoring (BGM) and professional continuous glucose monitoring (CGM).
DISCOVERY LEARNING FROM STRUCTURED BGM
Both of us spent a large portion of our career in the primary care setting where we routinely used structured BGM.There are 3 profiles that we have routinely used with clients/patients to help them to discover and learn about their blood glucose patterns and how favorite foods and physical activity affect them. We call this “discovery learning” because on their own, using “personal experiments” people are uncovering aspects of their diabetes themselves. And when people learn by doing, they are able to make health decisions that work for them. They are identifying “what’s working well” and are able to apply solution focused tactics to “do more of what’s working” and focus on successes instead of problems. Discovery learning is a great way to incorporate a solution-focused approach into practice. Let’s look at some examples
When using BGM there are several profiles or checking patterns you can apply.
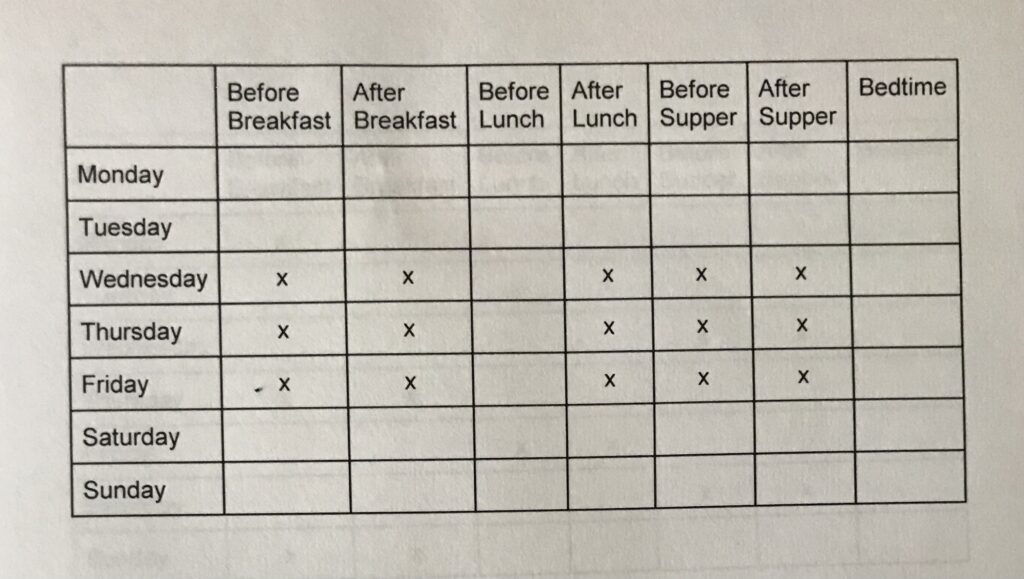
7-point profile
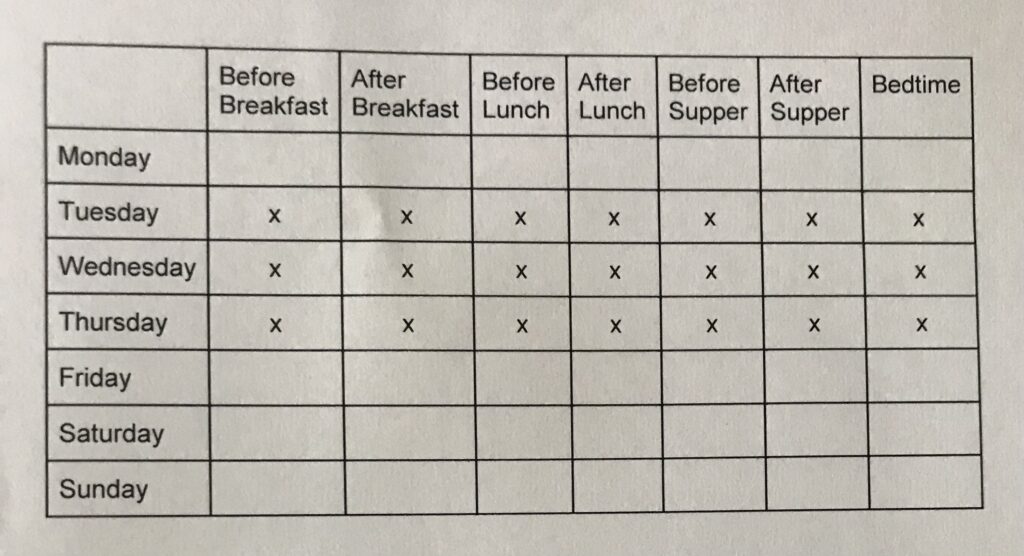
This one can be helpful to use for 3 days prior to a visit, for instance. This profile uses 21 strips, or 7 checks (before and after each meal and at bedtime) 3 days in a row. See the table below. The concentrated focus helps to measure the magnitude and frequency of short term fluctuation in blood glucose. It can be helpful in reducing the therapeutic inertia (Read more about therapeutic inertia in our blog here.)
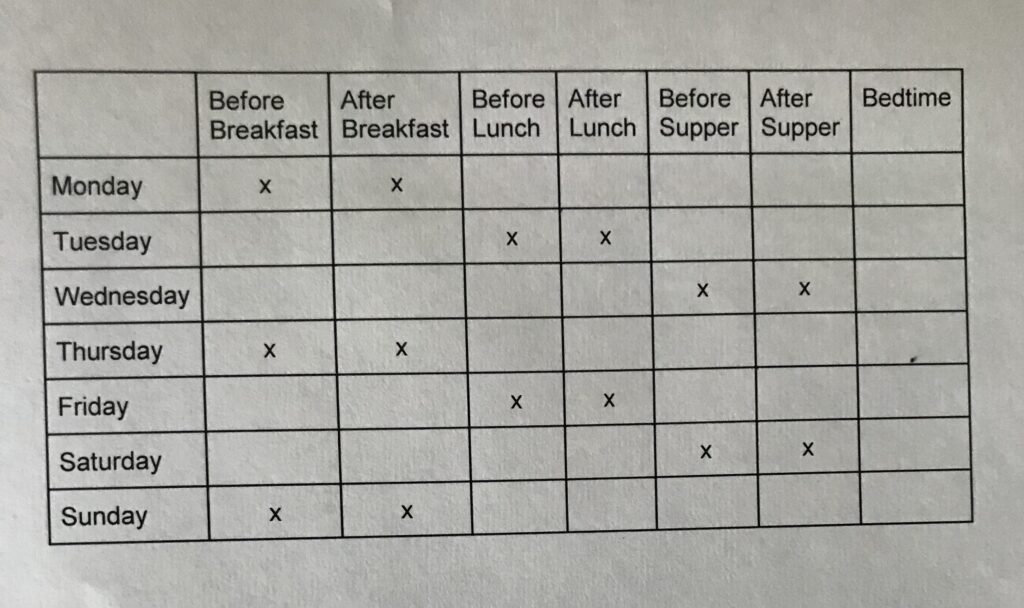
5-point profile
Similarly is the 5-point profile which requires fewer strips (15), if supply of adequate test strips is a concern. The 5-point profile includes 5 checks daily for 3 days, as you see in the table below – checking before and after breakfast and supper, as well as after lunch.
Paired checking
This is one of our favorite profiles for discovery learning. It can be used to focus on one thing, such as how a food/meal impacts blood glucose. We’ve had many clients/patients use paired checking to learn how their Friday night pizza affects their blood glucose. One example that stands out was an individual who routinely ate ½ of a medium hand-tossed pepperoni pizza (4 slices). After seeing the spike in his blood glucose, he decided to go with 2 slices and a side green salad, and saw his blood glucose fall back into range. We encourage patients to conduct their own “experiments”, if you will, to learn how food (type, portion) or adding in more physical activity affects them.
Paired checking can also be used around 1 meal time each day, rotating amongst the meals over the course of the week, to give a good look at blood glucose patterns.
Follow-up on personal experiments
At the follow-up to see what the individual learned from structured BGM, ask solution-focused questions in a non-judgemental way, such as:
I know you really like cheesecake and were planning to try paired checking to see how 3 bites satisfied you and affected your blood glucose, as compared to eating a whole piece. What did you learn? Did that change your plans? What are some options if your glucose spikes?
What have you learned during your discovery? And follow up with, How can you do more of that?
DISCOVERY LEARNING FROM PROFESSIONAL CGM
Another tool available to support people with type 2 diabetes to engage in discovery learning is by using professional CGM. Professional CGM is owned by the clinic, not the person with diabetes, for intermittent CGM use. Similar to the personal experiments described with BGM, a person can choose to view their data before and after favorite foods, different activities, or even before and after sleep or a stressful event. The benefit of professional CGM is that the individual doesn’t have to do a fingerstick as the unblinded professional CGM can be connected to their smartphone and they are able to see their data in real time for up to 10 days. We’ve written about discovery learning and CGM previously. There is also a blinded professional CGM where the person reviews the data at the end of session retrospectively. While not as useful for discovery learning and personal experiments, if they keep good records of food and activity they can identify trends and patterns.
Examples of personal experiments:
Favorite foods – While wearing the CGM your client might decide to eat different breakfasts each day of the week, and view their data on their smartphone before and again two hours later to see if they stayed in their target range (typically 70mg/dL-180mg/dL). They might choose their favorite high carb breakfast one day, and then a low carb version the second day, and then something in-between the next day.The beauty of personal experiments is that they can be anything that matters to the person.Through this personal discovery, they are able to learn what is working and make decisions.regarding their next steps.
Physical activity – Similar to evaluating the impact of food on glucose values, the same can be done for physical activity. The client can check their smartphone to know their glucose value and their trend arrow direction (are they staying steady, trending up or down) and then choose a variety of physical activities to evaluate the impact. Some questions they may ask are: What happens when I start physical activity when I have a trend arrow going down but my glucose is in range? Or what happens when I complete my physical activity and my trend arrow is going up? Many people discover that their glucose values actually increase following physical activity, but then come down later and using CGM can help them to plan how they respond.
Stress – Using CGM can really help clients understand the impact stress can have on their glucose. We’ve shared in our presentations about a friend who’s CGM values went straight up during a stressful event when she had nothing to eat or drink (the fire alarm went off, she ran out of her condo but forgot to get her cat …good news in the end it was a false alarm and the cat was fine!). Viewing data during stressful times can help people remove some of the guilt they experience with glucose fluctuations and help them to realize that diabetes is a challenging condition to manage.
Follow-up on personal experiments
Similar to BGM, use your solution-focused tools when discussing data. Focus on what went well, what the individual learned, and remember that all data are valuable. Data are just numbers and not judgements and do not define a person as “good” or “bad.” Help your clients value data to support their learning and to modify their health behaviors, even when their choices may not be choices you would suggest. People need to be ready to make big changes, and over time, data can help them get there!
I see you changed how much you walked after dinner, what did you learn?
You were in target range after these three meals, how did you do that? How can you do more of that? And what else?
We’ve written before about the 42 different factors that affect glucose (see Bright Spots and Landmines) and how Bright Spots are very similar to “exceptions” in a solution-focused approach, a time when things are going well. Author Adam Brown mentions that he would not have been able to identify these 42 factors without the use of CGM to guide him and reveal glucose changes that were unknown before. There is nothing more helpful for someone trying to make a challenging health behavior change than personal data to help them identify what they can do and what is reasonable for them.
Stop back by in 2 weeks when we’ll share a sneak peek at our session we’ll be presenting at the ADCES22 conference in Baltimore, MD!
We welcome anyone interested in our approach to Subscribe to our blog and we’ll email you when a new post is published!
If you are a health care professional and interested in learning more about our solution-focused practice and approach, when you subscribe to our blog, we’ll send you in return a FREE resource of 10 Solution-Focused Questions to start a solution-focused discussion with your clients.
Follow us on Twitter and Instagram @AFreshPOVforYou
Deb is employed by Dexcom, but her words and opinions in this blog are her own.
Tami is employed by the University of Kentucky HealthCare Barnstable Brown Diabetes Center, but her words and opinions in this blog are her own.
“The secret of living well and longer is: eat half, walk double, laugh triple, and love without measure.” ~ Tibetan Proverb
As we revisit our series on transforming primary care encounters, we’d like to take a step back, if you will, to the diagnosis of prediabetes. In our clinical experience there is a vast difference in these early conversations in the health care setting – sometimes a stern warning to change habits “or else”, to almost no recognition of the elevated blood glucose at all, with no discussion about the potential risk of developing type 2 diabetes. Deb discovered that both of her parents had been living with prediabetes for years, but neither of them had even been told of their lab levels except, “things look good.” As with a new diagnosis of type 2 diabetes, we believe that incorporating a solution-focused approach with a prediabetes diagnosis is equally as important.
If you’ve read our previous blogs you know that a solution-focused approach is the opposite of a more traditional “problem-focused” approach. The goal is to help the individual recognize exceptions (times when their problems did not happen) and help them to focus on health behavior changes by doing “more of what works.” How can we use this approach in the prediabetes conversation?
Using a solution-focused approach at the prediabetes diagnosis conversation
The ADA 2022 Standards of Medical Care indicate that screening for prediabetes should start at age 35, but earlier for those with risk factors. We are advocates that everyone who meets the criteria for a prediabetes diagnosis deserves the information as early as possible so they may decide what types of health behavior changes they are willing and able to make. Thus, using a solution-focused approach from the beginning is critical to set the stage for a lifetime of ongoing conversations. A clinician’s approach to this conversation can make the difference in early action to help prevent or delay type 2 diabetes – and thus potential prevention of long-term complications, reduction in medication, and living a healthier life.
Current guidelines suggest enrolling individuals with prediabetes into a National Diabetes Prevention Program (DPP) given DPP study outcomes that showed a 58% reduction in risk of progression to type 2 diabetes with lifestyle intervention. Research shows that participants who lose 5-7% of their body weight and add 150 minutes of exercise per week cut their risk of developing type 2 diabetes by up to 58% (71% for people over 60 years old).
The guidelines also recommend metformin for those with a higher BMI, higher A1C, and history of gestational diabetes. Since many don’t want to take medication, there is a great need for open discussion from the beginning to use shared decision-making to lay out the facts, what is known, what the research indicates, and their overall level of risk.
We know that patients (clients) greatly value what their primary care provider (PCP) recommends to them, so having these open discussions can help the PCP identify what the individual is willing and able to do. If they might benefit from medication, and are likely to be challenged to engage in physical activity or choose more healthful foods, then medication might be a beneficial option. It’s important to balance goals from the PCP perspective against the capacity of the person with the new diagnosis. Asking questions and engaging in problem-free talk can be more impactful than giving a list of instructions. Maybe you simply state, “I know this is hard to hear, how can I help?” and “What information would you like to hear from me today as you start to learn about prediabetes?”
As we shared in our type 2 diabetes diagnosis blog, the American Diabetes Association encourages four critical conversations that promote “early positive conversations about the nature of diabetes.” We believe that applying this during the prediabetes diagnosis can be equally as valuable. These conversations address many tenets we value in a solution-focused approach, including person-centered, strength-based language, problem-free talk, listening, and building a partnership with clients.
4 critical conversations
There are four critical conversations that need to happen early in the diagnosis. We’ve modified these questions to fit prediabetes and encourage you to build upon these questions at each visit. Start small with a few comments and then build upon them as the person is learning to accept the diagnosis and is ready to learn more. At diagnosis, conversation #1 is the most significant. (adapted from ADA Overcoming Therapeutic Inertia)
Prediabetes may progress to type 2 diabetes over time, as your body’s insulin production changes.
I want you to know that prediabetes is an opportunity to make health behavior changes that may prevent or delay type 2 diabetes. However, it’s important to know that even if you follow every guideline you may still develop type 2 diabetes.
Your treatment plan will change over time as your prediabetes changes.
You may need to add a medication as your prediabetes changes. This is not a personal failure, just a part of how the progression to diabetes may happen.
You can’t do this alone.
I am here to help you.
Share your difficulties with following diabetes prevention guidelines.
Managing prediabetes day in and day out can be hard. Share anything that may be getting in the way of managing your diabetes and also share your successes.
On a scale of 0-10 where zero is no stress and 10 is the worst stress you’ve ever experienced, where are you right now?
Use their answer to finish the visit and provide one action for them to focus on.
If 0-4: Encourage doing some research online at trusted sources like the ADA, CDC or ADCES.
If 5-7: Identify one strength they already have and build upon it
What is one thing you do for yourself every day that makes you feel healthy? How can you do more of that?
If 8-10: just encourage them to breathe and take some time to let it sink in and to come back with questions in one week
I know how hard this can be, take some time, write down questions you have, and let’s meet and talk more next week.
Create a supporting environment
Reinforce that small changes can help move them in the right direction, and that you don’t expect perfection. If they do the best that they can do, that’s the best they can do. Remind them that you are partners on this journey. We believe that creating a supportive environment from day one, can empower people to learn to live with their diabetes.
Stop back by in 2 weeks as we wrap up our series on incorporating a solution-focused approach when managing type 2 diabetes in the primary care setting. We’ll focus on interpreting diabetes data in primary care in a solution-focused way.
We welcome anyone interested in our approach to Subscribe to our blog and we’ll email you when a new post is published!
If you are a health care professional and interested in learning more about our solution-focused practice and approach, when you subscribe to our blog, we’ll send you in return a FREE resource of 10 Solution-Focused Questions to start a solution-focused discussion with your clients.
Follow us on Twitter and Instagram @AFreshPOVforYou
Deb is employed by Dexcom, but her words and opinions in this blog are her own.
Tami is employed by the University of Kentucky HealthCare Barnstable Brown Diabetes Center, but her words and opinions in this blog are her own.
Success is built sequentially. It’s one thing at a time. – Gary W. Keller
Building on our last blog about how to have a productive type 2 diabetes (T2D) diagnosis conversation using a solution-focused approach, NOW let’s focus on how to incorporate these techniques into follow up visits. These follow-up visits are ideally “diabetes only” visits. In a brief primary care visit that is addressing multiple issues, it can be too challenging to focus on specific diabetes priorities. The American Diabetes Association recommends scheduling “diabetes only” appointments to focus on and address diabetes-related concerns. This diabetes only visit is an opportunity to be a think partner with your client to answer questions, address concerns, and map out a plan together.
Using a solution-focused approach at a “diabetes only” visit?
Since asking eliciting questions is a primary tenet of a solution-focused encounter, we encourage starting all visits by listening and learning from your client. Even though the client is new to diabetes, they are the expert in that they know what works in their life in other aspects, and they know what they are capable of doing now. (Read more about experts here)
The goal is to focus on things that are working well, and when something works, do more of it! Help your clients to recognize their strengths by identifying exceptions. We’ve written about exceptions here). “Diabetes only” visits can be structured in a systematic way.
10-step model for a “diabetes only” visit
Start with a question.“I’m looking forward to hearing how things have been going since our last visit. Can you tell me one thing that went well for you this past week (or since we last met)?”
Explore the reply further. “How do you think you can do more of (that)?”
Personalize. “I want to make sure this visit is successful for you, what do you need to know or learn by the end of the visit?”
Empower. Empower people with diabetes with tailored education and support to ensure their questions, needs and desires are met.
Set a SMART goal. A SMART goal helps move the individual towards the direction they want to move based on your conversation. It helps quantify progress with measurable steps and keeps things reasonable and achievable.
Ask a scaling question. “On a scale of 0-10 where zero is never and 10 is all the time, how confident are you that you can achieve your goal?
Use their answer to finish the visit and provide one action for them to focus on.
If 0-4: Encourage them to revise their smart goal, it might be too difficult to achieve.
If 5-7: Identify one strength they already have and build upon it. “What is one thing you do where you feel confident in your actions? How can you do more of that?”
If 8-10: Encourage them to challenge themselves and consider a goal that might move them closer to their overall health behavior outcomes.
Review the four critical conversations. As we discussed in the last blog, we encourage you to build upon these conversations at each visit. (adapted from ADA Overcoming Therapeutic Inertia)
Conversation 1: The nature of T2D is to change over time, as your insulin production changes.
“Although diabetes is progressive, and can change over time, your actions can make a difference in slowing the progression over time.”
Conversation 2: Your treatment plan will change over time as your diabetes changes.
“We will work with you to find a treatment plan that achieves health goals while also considering your preferences and values.”
Conversation 3: You can’t do this alone.
“Seek help from family, friends and community support resources.”
Conversation 4: Share your difficulties with managing your diabetes.
“Your healthcare team is on your side and we will support you in whatever ways you need to manage your diabetes”
Refer for diabetes self-management education and support.
Thank them for coming in and for working hard.
Plan follow-up. Plan the next diabetes only visit.
Join us next time as we continue our series on incorporating a solution-focused approach when managing T2D in the primary care setting. We’ll continue to help you build your solution-focused tool-kit. Our goal is to start slow and share small, achievable bite-size practice changes you can implement over time.
We welcome anyone interested in our approach to Subscribe to our blog and we’ll email you when a new post is published!
If you are a health care professional and interested in learning more about our solution-focused practice and approach, when you subscribe to our blog, we’ll send you in return a FREE resource of 10 Solution-Focused Questions to start a solution-focused discussion with your clients.
Follow us on Twitter and Instagram @AFreshPOVforYou
Deb is employed by Dexcom, but her words and opinions in this blog are her own.
Tami is employed by the University of Kentucky HealthCare Barnstable Brown Diabetes Center, but her words and opinions in this blog are her own.
“Health is a state of body. Wellness is a state of being.” ~ J. Stanford
Our prior post in our series on transforming primary care encounters focused on combating therapeutic inertia. Today, we’d like to start from the very beginning – the conversation when the client first learns they have type 2 diabetes (T2D). When beginning diabetes conversions using a solution-focused approach, we believe you will find that your relationship with your clients can improve and it will create an opportunity for ongoing shared decision-making.
As a reminder, a solution-focused approach is the opposite of a “problem-focused” approach. The goal is to help the person with T2D recognize exceptions (when their problems did not happen) and help them to focus on their health behavior changes by doing “more of what works.”
Using a solution-focused approach at the T2D diagnosis conversation?
When preparing for the diagnosis conversation, first put yourself in your clients shoes. How would you want the conversation to go? What would you want to hear? Also consider your body language, your tone and word choice. We know in a busy primary care office, so much time is spent documenting in the EHR, but for this very important discussion, take a moment and step away from the computer, lean in to your client, show empathy and compassion while you say some very important words. Many are overwhelmed when they hear the news that they have T2D, and often won’t hear much of the rest of the conversation. Ask questions and engage in problem free talk, instead of giving a list of instructions. Maybe you simply state, “I know this is hard to hear, how can I help?” and “What information would you like to hear from me today as you start to learn about T2D?” Consider making this appointment brief and bring them back for a follow up “diabetes only” visit once they have time to absorb and process the information.
To build upon our blog on therapeutic inertia, we’re including some impactful information from the American Diabetes Association that encourages four critical conversations that promote “early positive conversations about the nature of diabetes.” These conversations address many tenets we value in a solution-focused approach, including person-centered, strength-based language, problem-free talk, listening, and building a partnership with clients.
4 critical conversations
There are four critical conversations that need to happen very early in the diagnosis. We encourage you to build upon these questions at each visit. Start small with a few comments and then build upon them as the person is learning to accept the diagnosis and is ready to learn more. At diagnosis, conversation #1 is the most significant. (adapted from ADA Overcoming Therapeutic Inertia)
The nature of T2D is to change over time, as your insulin production changes.
“I want you to know that diabetes is not a personal failure and it doesn’t mean you’ve done something wrong.”
Your treatment plan will change over time as your diabetes changes.
“You may need to add new medications as your diabetes changes. This is not a personal failure, just a part of how diabetes treatment progresses.”
You can’t do this alone.
“I am here to help you.”
Share your difficulties with managing your diabetes.
“Managing diabetes day in and day out can be hard. Share anything that may be getting in the way of managing your diabetes and also share your successes.”
“On a scale of 0-10 where zero is no stress and 10 is the worst stress you’ve ever experienced, where are you right now?“
Use their answer to finish the visit and provide one action for them to focus on.
If 0-4: encourage them to do some research online at trusted sources like the ADA, Diatribe, or ADCES.
If 5-7: identify one strength they already have and build upon it
“What is one thing you do for yourself every day that makes you feel healthy? How can you do more of that?”
If 8-10: just encourage them to breathe and take some time to let it sink in and to come back with questions in one week
“I know how hard this can be, take some time, write down questions you have, and let’s meet and talk more next week.”
Reinforce that small changes can help move them in the right direction, and that you do not expect perfection. If they do the best that they can do, that’s the best they can do. Remind them that you are partners on this journey. We believe that creating a supportive environment from day one, can empower people to learn to live with their diabetes.
Keep reading our series on incorporating a solution-focused approach when managing T2D in the primary care setting. Next time we will focus on the first follow up visit after diagnosis. Stop back by in 2 weeks as we share more tips to build your solution-focused tool-kit over time.
We welcome anyone interested in our approach to Subscribe to our blog and we’ll email you when a new post is published!
If you are a health care professional and interested in learning more about our solution-focused practice and approach, when you subscribe to our blog, we’ll send you in return a FREE resource of 10 Solution-Focused Questions to start a solution-focused discussion with your clients.
Follow us on Twitter and Instagram @AFreshPOVforYou
Deb is employed by Dexcom, but her words and opinions in this blog are her own.
Tami is employed by the University of Kentucky HealthCare Barnstable Brown Diabetes Center, but her words and opinions in this blog are her own.
Where you stand determines what you see and what you do not see; it determines also the angle you see it from; a change in where you stand changes everything. – Steve de Shazer, pioneer of solution-focused brief therapy
As we continue our series on transforming primary care encounters, today we’re tackling the topic of combatting therapeutic inertia.
What is therapeutic inertia?
In a general sense, “therapeutic inertia” is a lack of timely adjustment to the treatment plan when a client’s treatment goals are not being met. In the diabetes management arena, therapeutic inertia means being slow to add or change the care plan if a client’s A1C is above target. Delays in implementing the most effective care for each person with diabetes can happen at any phase of diabetes treatment and can range for instance from referring for diabetes and nutrition education, to starting the first medication, or intensifying medication management, including starting insulin.
Why stop therapeutic inertia?
The evidence is clear on two things:
Managing glucose levels early in the course of diabetes leads to better long-term outcomes and reduces risk of complications.
Those who reach their A1C targets soon after they’re diagnosed with diabetes are more likely to keep their glucose in target.
This is such a timely and impactful topic that ADA has launched an initiative called Overcoming Therapeutic Inertia. There are many resources for primary care clinicians to learn practical tips to focus on diabetes care in a proactive, timely way to improve outcomes. Learn more here.
Does shared decision making play a role?
One key tenet of shared-decision making is that all care decisions are discussed together with the client, and decisions are made together, which will ultimately mean more people with diabetes are following their treatment plan. Research shows us that when people are not involved in their diabetes medication decisions, they often no longer take the medicine.
When we talk about therapeutic inertia we are addressing both the clinician reluctance to advance therapy and the client’s reluctance to follow through with prescribed therapy. When we add shared decision-making we remove some of the barriers to medication taking. We discuss the potential side effects of the medication, costs, schedule and impact to their lifestyle. These are important decisions that need to be understood for individuals to embrace new therapy.
So how does incorporating a solution-focused approach address therapeutic inertia?
A solution-focused approach that encourages shared decision-making can be a tool to overcome inertia. As we’ve discussed previously, incorporating a solution-focused approach removes the shame and blame often associated with diabetes. When you discuss the clients goals and outcomes and what is working well for them, together you can identify the best therapy.
A solution-focused approach is a questioning approach, asking questions allows you to delve down to identify what is most important. An example of a medication-related question might be: What is most important to you when choosing a medication, the potential of weight gain or the need to check glucose before meals? ”And what else?” questions can be incorporated to learn more.
Since asking eliciting questions is a primary tenet, we encourage you to start all visits by listening and learning from your client. Remember, the client is the expert (read more about experts here), and even though they may be new to diabetes, they know what works in their life in other aspects, they know what they are capable of doing now.
When incorporating a solution-focused approach, each person will map out their own successful plan based on their lives, needs, strengths and desires. The care plan becomes personalized and directly relevant to the client. If something works, do more of it, help them recognize their strengths by identifying exceptions ( written about exceptions here.)
This solution-focused shared decision-making can build relationships and guide clients towards achieving goals, thus overcoming therapeutic inertia.
Next up
Join us next time as we continue our series on incorporating a solution-focused approach when managing T2D in the primary care setting. We’ll visit the moment of diagnosis with diabetes and share tips/tactics you can use to continue to help you build your solution-focused tool-kit.
We welcome anyone interested in our approach to Subscribe to our blog and we’ll email you when a new post is published!
If you are a health care professional and interested in learning more about our solution-focused practice and approach, when you subscribe to our blog, we’ll send you in return a FREE resource of 10 Solution-Focused Questions to start a solution-focused discussion with your clients.
Follow us on Twitter and Instagram @AFreshPOVforYou
Deb is employed by Dexcom, but her words and opinions in this blog are her own.
Tami is employed by the University of Kentucky HealthCare Barnstable Brown DIabetes Center, but her words and opinions in this blog are her own.
If it ain’t broke, don’t fix it. Once you know what works, do more of it. If it’s not working, do something different. – Steve de Shazer and Insoo Kim Berg, pioneers of solution-focused brief therapy
Our last blog spotlighted the power of words and using person-first, strengths-based language in diabetes related conversations in primary care. As we continue our series on transforming primary care encounters by incorporating solution-focused techniques, maybe your interest is piqued by this new approach, but you’re not quite sure how to begin to incorporate it into your practice? Today we share 7 practical tips to get started.
1 – Ask “exception” questions. Exceptions are times when an expected problem does not occur. These are times we want to identify, focus on, and encourage the client to explore. These exceptions help the client move towards their desired future. Here are 2 examples of “exception” questions:
You mentioned that you typically struggle to be physically active in the evenings but you were able to go to the gym after work last week? How did you manage to do that?
Cooking meals at home has been a challenge for you, yet you cooked two times last week. What changed to allow you to make that happen? And what else?
2 – Use person-first, strengths-based language. This may seem simple, but is hugely impactful. This means using language that is neutral, non-judgmental, and free from stigma. Language that is inclusive, respectful, and imparts hope. Word choice that fosters collaboration with your client and is person- centered. Focusing on language can remove the stigma associated with diabetes.
3 – Practice problem-free talk. By incorporating this one impactful change you will already notice how the quality of visits and client engagements will improve – building the therapeutic relationship, hope, and motivation. The conversation at the beginning of an encounter is critical to build the therapeutic relationship. By starting the conversation with the goal of the client, you acknowledge that you are focused on their needs and desires and are committed to helping to meet their goals. Two great ways you could begin a visit are to ask your client:
What would make this a successful appointment for you?
At the end of this visit, what would you need to know/learn to say this was worth your time?
4 – Ask the Miracle Question.
The Miracle Question applied to diabetes is one tool or technique in a solution-focused tool-box to help clients envision a future that is more problem-free.
Miracle Question: If you could fast-forward to a time where you feel satisfied with your diabetes management, what will be different in your life that will let you know things are better?
You can learn more about the Miracle Question applied to diabetes in a previous blog post here. The Miracle Question helps people identify those “exceptions” mentioned in #1. The Miracle Question challenges a person to look past their obstacles and feelings of hopelessness to focus on possibilities, opportunities, and a vision for the future. The goal is to help one identify what they’ve actually known all along, and that they have the power to make choices and changes that can move them forward. By focusing on “exceptions”, goals become different. Focus turns to what is desired in our life instead of what “won’t happen” anymore.
5 – Ask eliciting questions. When incorporating a solution-focused approach you need to ask eliciting questions to uncover solutions and guide the individual. It is key that these questions are open-ended and help the individual see how they can be successful. Instead of asking questions that focus on the problems (since living with a chronic condition cannot benefit from a “quick fix”), instead, explore their strengths and resources they already possess and how those resources can apply to their diabetes management.
What has been going well since I last saw you?”
That one question can start the visit on a positive note, acknowledge the work that it took to accomplish that, and then leverage how the client can continue those positive behaviors and build on them for future health success. Questions can also focus on details when the person identifies a success:
How exactly did you do that? What exactly did you do differently?
6- Ask future visioning questions. These questions can focus on the short-term or long-term views of the client’s preferred future. These questions help the individual realize that solutions are possible and help them see their desired future state. As you recall one of the key tenets is the client is the expert about their own life and their own diabetes. (Read more about experts here)
What would you like to see yourself doing in the next (day, week, month) to move you forward towards your goals? And what else?
Following up with “what else?” encourages people to dig deeper and think through in detail what they are capable of.
7 – Use scaling questions. Scaling questions are a great tool to move away from all or nothing thinking. They focus on progress, motivation, and confidence.
On a scale of 0-10 where 0 is not confident at all and 10 is very confident, how much confidence do you have that you can meet your goal to (insert personal goal here)?
If less than a 7, follow up with one of these:
What could move you to a 7?
What would need to happen to move you one number higher?
What would one number higher look like?
How would others notice you’re more confident?
How come you’re not at a lower number? How did you do that?
Keep reading our series on incorporating a solution-focused approach when managing T2D in the primary care setting. Our next blog will focus on therapeutic inertia. Curious what that means? Stop back by in 2 weeks as we share more tips to build your solution-focused tool-kit over time.
We welcome anyone interested in our approach to Subscribe to our blog and we’ll email you when a new post is published!
If you are a health care professional and interested in learning more about our solution-focused practice and approach, when you subscribe to our blog, we’ll send you in return a FREE resource of 10 Solution-Focused Questions to start a solution-focused discussion with your clients.
Follow us on Twitter and Instagram @AFreshPOVforYou
Deb is employed by Dexcom, but her words and opinions in this blog are her own.
Tami is employed by the University of Kentucky HealthCare Barnstable Brown DIabetes Center, but her words and opinions in this blog are her own.
The language for solution development is different from that needed to describe a problem. Steve de Shazer, pioneer of solution-focused brief therapy
If you are just catching up on our thoughts around transforming primary care visits by incorporating solution-focused (SF) tools and techniques, check out our last post about the benefits of using a SF approach. This week in our series we are spotlighting the power of words – meaning the words that we choose in conversations and interactions with clients. As the authors of the transformative paper The Use of Language in Diabetes Care and Education(Diabetes Care 2017;40:1790–1799 | ) call out:
“Words are immediately shaped into meanings when people hear or read them, and those meanings can affect how a person views him or herself…Words have the power to “elevate or destroy”.”
Person-first, strengths-based language
We’ve written extensively about the power and benefit of using person-first, strengths-based language in diabetes care and education and how #languagematters. Research clearly shows that positive language is associated with positive health outcomes. And on the flip side, when people are faced with language that is judgemental, blames and shames, they are less likely to share openly with their healthcare team.
3 examples of how flipping a few words can flip the conversation:
Refer to one as a “person with diabetes”, rather than a “diabetic” (which labels them).
Refer to “check” blood glucose, rather than “test” blood glucose” (which implies good/bad or pass/fail)
Describe the scenario such as, “You take your medicine about half the time.”, rather than labeling one “noncompliant” (which shames)
A SF approach is not possible unless there is open communication facilitated by strengths-based language.
Why does language matter in primary care?
Again, language is powerful. We’ve discussed that the relationship between the healthcare provider (HCP) and the client is different. Instead of a hierarchical position, in SF relationships, the HCP and the client are considered “think partners”. They work together to identify solutions to move that individual forward towards achieving their goals. Thus, the language must follow to build the relationship.
Importantly, the goal for those with type 2 diabetes (T2D) is to feel they are part of a partnership in their diabetes management with their HCP, where they can discuss their challenges and their strengths and work together. Is it possible to create and strengthen this relationship when words such as non-compliant, cheating, not working hard enough, or other shaming and blaming words are used?
When we use words that focus on what people “can do”, and words that describe their actions, we recognize and acknowledge that diabetes is managed by the person living with it and we acknowledge that it’s one piece of their life and not their whole life. When a person living with diabetes engages with their primary care team as a partner, much can be accomplished. As we’ve noted before, you are able to “flip” the conversation from a negative to a positive and foster that “think partner” relationship.
Imagine a situation where an individual living with T2D looks forward to their primary care appointments because they are going to share with and learn from their HCP with no fear of judgment. They’ll talk about their struggles and challenges in a truthful manner and together they’ll identify areas that are working and small steps that can be taken to lead towards success.
The most important lesson you can take away from this discussion is that using strengths-based language is actually easy to do. As our friend and colleague Jane K. Dickinson says, “when you put the person first (not the diabetes), the language will follow.”
Our goal is that people living with T2D will develop a positive relationship with their primary care team, and all involved will understand the challenges, the opportunities, and the need for an empowering approach towards diabetes care and education. And we believe that a change in language can lead that.
If you’re not sure how to begin, consider starting your next encounter with one of these questions:
Thanks for coming in today. What’s been going well for you in your diabetes management?
It’s so nice to see you today, managing diabetes is really hard work – it’s like a part-time job. Tell me what you’ve been happy/pleased with about your diabetes management since we last met?
We all need support in some manner. Diabetes is a team effort. How can I support you and support the changes you want to make? I’m here for you.
We hope you’ve been learning little nuggets with each blog post as you build your solution-focused tool box for managing T2D in primary care. Keep reading our series on incorporating a solution-focused approach when managing T2D in the primary care setting. Our goal is to start slow and share small, achievable, bite-size practice changes you can implement over time.
We welcome anyone interested in our approach to Subscribe to our blog and we’ll email you when a new post is published!
If you are a health care professional and interested in learning more about our solution-focused practice and approach, when you subscribe to our blog, we’ll send you in return a FREE resource of 10 Solution-Focused Questions to start a solution-focused discussion with your clients.
Follow us on Twitter and Instagram @AFreshPOVforYou
Deb is employed by Dexcom, but her words and opinions in this blog are her own.
Tami is employed by the University of Kentucky HealthCare Barnstable Brown Diabetes Center, but her words and opinions in this blog are her own.
Once you know what works, do more of it. – Steve de Shazer and Insoo Kim Berg, pioneers of solution-focused brief therapy
As we continue our new series on transforming primary care encounters by using a solution-focused approach, today let’s talk about the benefits of this approach. Benefits to you as a health care provider and more importantly benefits to your clients. We’ve had several primary care providers encourage us to share more on this approach as they found it to be a transformational way of thinking and engaging with clients.
What are the benefits to the client?
Without a doubt, managing diabetes is complex and burdensome. In 2019, we conducted a qualitative research study with Twitter Chat data from a #DSMA chat we moderated around a solution-focused tool called “The Miracle Question”. We first presented these findings in 2019 at the 55th Annual Meeting of the European Association for the Study of Diabetes Conference in Barcelona, Spain. Two compelling comments from participants with diabetes that came out of that study.
“Diabetes interrupts my life… every minute.”
“Success would look like people realizing what diabetes is and we can stop with these assumptions and jokes about diabetes.”
As we’ve written about many times, individuals that live with type 2 diabetes (T2D) have many obstacles to overcome due to the lack of understanding about the condition.We know that T2D has a genetic link and is more common in individuals of color, those with a family history, and that risk increases with aging. While making more healthful behavior changes is critical to living a healthy life, the genetic nature of the condition is not well known in the general community and not discussed enough in medicine, the community at large, and the media.
The goal is to help the person with T2D recognize exceptions(a time when their problem does not happen) and help them to focus on their health behavior changes by doing “more of what works.” Give our previous blog here a quick read to get up to catch up on the basic tenets of the solution-focused approach and how implementing an approach that focuses on solutions instead of problems can “flip” the conversation in primary care and build stronger relationships.
Ultimately, developing stronger relationships will facilitate positive discussions about therapy including medication, food choices, physical activity and more.
What are the benefits to the provider?
Brief intervention. One of the most important benefits of incorporating a solution-focused approach in primary care is that it is a “brief” intervention. With often many competing demands to address during a primary care encounter, you do not need to delve deep into problem-solving mode. Instead you discuss what’s already working well and step alongside the client as a “think partner” to do more of what “works.”
Ownership transferred to the client. Ideally a solution-focused approach incorporates questions to generate discussion (we’ll share some of these in a future post). . In this way, the primary care provider helps the client elicit “change talk” instead of “telling” the client what to do. Tami had a client this past week that said those very words… “I really like that you’re not telling me what to do, but spending time talking to me and brainstorming ideas so I can decide what I want to do.” The client will have ownership over their decisions and be more invested in the next steps. This is really the first step in shared decision-making.
Greater individualization of care. The recent 2022 ADA Standards of Care presents much greater emphasis on individualization and personalization of care. What better approach to individualize the care plan than asking the individual what is working for them and what they think might be the best next steps. Together you can identify small steps towards their goals.
Come back in two weeks for our thoughts on the power of language when managing T2D in the primary care setting. We’ll re-introduce the concept of person-first, strengths-based language and use in a solution-focused approach with tips for the primary care team, both clinician and person with diabetes. We’ll continue to help you build your solution-focused tool-kit over time.
We welcome anyone interested in our approach to Subscribe to our blog and we’ll email you when a new post is published!
If you are a health care professional and interested in learning more about our solution-focused practice and approach, when you subscribe to our blog, we’ll send you in return a FREE resource of 10 Solution-Focused Questions to start a solution-focused discussion with your clients.
Follow us on Twitter and Instagram @AFreshPOVforYou
Deb is employed by Dexcom, but her words and opinions in this blog are her own.
Tami is employed by the University of Kentucky HealthCare Barnstable Brown DIabetes Center, but her words and opinions in this blog are her own.